
“Non-Binary” — The Gateway to Public Health Insurance Funding for the Sexless Barbie Body
Which procedures carried out under the label “non-binary” are intended to be funded by all of us in future


“I don’t want other vulnerable girls and women to go through what I went through,” said 36-year-old Camille Kiefel, after reaching a confidential settlement with her providers just days before her trial was set to begin in January 2026. Kiefel, who had identified as non-binary since 2015, underwent a mastectomy in 2020 at the age of 30. Two social workers had issued her referral letters after a single telehealth appointment each lasting under an hour. She received the letters despite a documented history of trauma, depression, suicidal ideation and ADHD, and despite being on long-term disability at the time of the surgery. Her distress did not improve. She has suffered permanent physical and psychological harm ever since.[1]
Just a few weeks earlier, Fox Varian had become the first detransitioner to win a jury verdict in New York, being awarded $2 million in damages for a mastectomy she had undergone at the age of 16.[2]
Recently, the American consumer protection agency, the Federal Trade Commission (FTC), filed a lawsuit against WPATH — the World Professional Association for Transgender Health. The organisation had, it alleged, provided medical providers with arguments designed to make false and unsubstantiated claims to parents, through which experimental and harmful procedures were financed and performed on children.[3]
The US cases are relevant to Germany
The rising tide of litigation in the United States offers a perspective for Germany: once young people and families harmed by transgender procedures stop staying silent and take legal action against doctors, psychologists, clinics and professional associations, the ideological culture of silence around transgender interventions will be broken. WPATH’s guidelines — developed in the United States — have had a direct influence on German clinical guidelines. What courts decide in the US therefore has an indirect bearing on Germany.
The personal background to my investigation
In Germany, Sabine Maur — former Vice-President of the Federal Chamber of Psychotherapists — is currently bringing legal proceedings against me. The next hearing is next week — on 9 July — before the Berlin Court of Appeal (Kammergericht). My goal remains to resist being silenced in my open criticism of gender-affirming procedures. I have used these proceedings as an occasion to investigate the subject of “non-binary” more closely.
In Part 1, I set out that “non-binary” is an ill-defined, activist term that is nevertheless intended to unlock statutory health insurance coverage for medical procedures. I also explained how Federal Health Minister Warken has instructed the Federal Joint Committee (G-BA) by administrative order to bring treatments for non-binary persons into the reimbursement system of the statutory health insurance (GKV) — while bypassing the benefit assessment procedure that the Federal Social Court (BSG) explicitly identified as the competent procedure in 2023.[4]
Part 2 answers the question: exactly which procedures are intended to be funded through health insurance under the label “non-binary”?

Non-binary — the sexless body
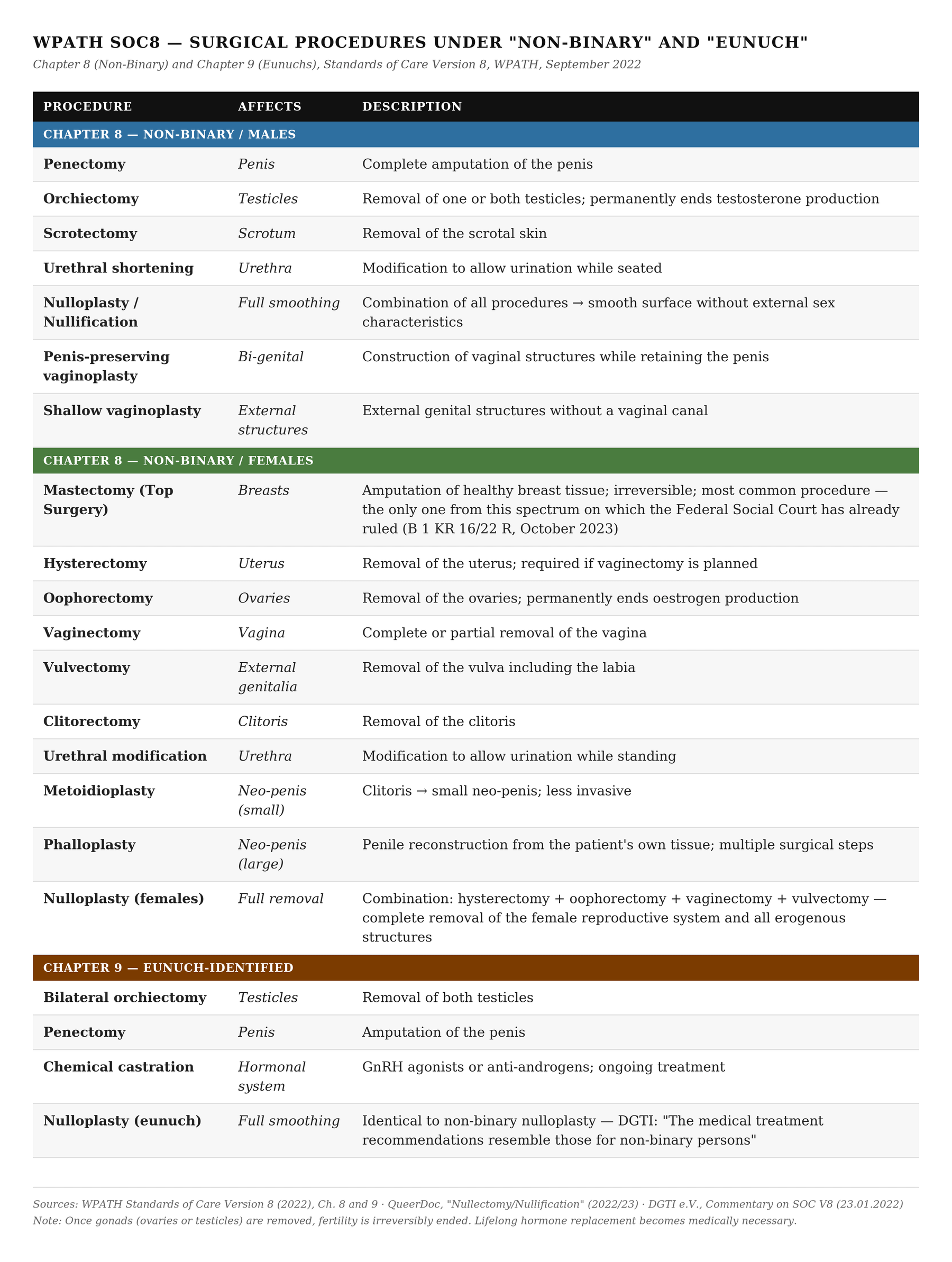
For gender-affirming procedures, the international organisation WPATH (World Professional Association for Transgender Health) regularly publishes guidelines that also serve as the basis for guidelines in Germany. The most recent version of the “Standards of Care” (SOC8, September 2022) introduced two new chapters: Chapter 8 “Non-Binary” and Chapter 9 “Eunuchs”. Neither chapter had appeared in any previous version.[5]
Chapter 8 lists specific surgical procedures for people who describe themselves as “non-binary” or “agender” — that is, neither male nor female. The ultimate goal is not to simulate the opposite sex, but to create a sexless body devoid of recognisable primary and secondary sex characteristics. This approach is called Nulloplasty.
The US-based health platform QueerDoc, which specialises in gender-affirming procedures, describes Nulloplasty as: the removal of internal and external genital structures with the aim of creating a smooth surface from the abdomen to the groin.[6] The glans tissue — the penile shaft or clitoris — can either be fully removed, preserved as a tactile protrusion, or “buried” beneath the skin to retain a centre of sensation without disrupting the smooth external appearance.
For males, Nulloplasty includes:
Penectomy: complete amputation of the penis
Orchiectomy: removal of the testicles
Scrotectomy: removal of the scrotal skin
Urethral shortening
WPATH SOC8 additionally recommends the following for this group under “non-binary”:
Penis-preserving vaginoplasty: construction of vaginal structures while retaining the penis
Shallow vaginoplasty: construction of external structures without a vaginal canal
For females, WPATH SOC8 lists the following procedures under Chapter 8:
Mastectomy (Top Surgery): amputation of both breasts — the most common procedure performed on girls and women who identify as non-binary or as trans men. It is the only procedure from this spectrum on which the Federal Social Court has already ruled (B 1 KR 16/22 R, October 2023 — more on this below). It is already available without GKV coverage at several clinics in Germany.
Hysterectomy: removal of the uterus (required if vaginectomy is planned)
Oophorectomy: removal of the ovaries (with or without hysterectomy)
Vaginectomy: removal of the vagina
Vulvectomy: removal of the external genitalia (partial or complete)
Clitorectomy: removal of the clitoris
Urethral modification
WPATH SOC8 also recommends the following for females under “non-binary”:
Metoidioplasty: clitoral enlargement following testosterone treatment, optionally with urethral lengthening
Phalloplasty: complex penile reconstruction using the patient’s own tissue (multiple surgical steps)
Complete Nulloplasty for females involves combined hysterectomy, oophorectomy, vaginectomy, vulvectomy and clitorectomy — in other words, the total removal of the female reproductive system and all erogenous structures.
All of these procedures are irreversible. They are performed on healthy bodies. Complications of this magnitude are not the exception but a routine part of medical practice: scarring, nerve damage, infections, chronic pain, loss of function. Recovery time, according to QueerDoc, is six to eight weeks — considerably longer for females due to the more extensive internal procedures.[7]
Non-binary = Eunuch
Alongside Chapter 8, WPATH has introduced a separate Chapter 9 in SOC8 for “eunuch-identified” persons. It defines this group as males who experience dysphoria regarding their male genitalia and seek their operative removal. Castration and penectomy are described as legitimate medical interventions — and as an innate constitution that can affect minors.
Feminist journalist Genevieve Gluck, in an investigative report, found that the Eunuch chapter had been directly influenced by castration fetishists and paedosadists who shared extreme sexual fantasies and footage — including recordings of gender-affirming procedures on boys — in eunuch forums. The Eunuch Archive forum is cited as a source in SOC8.[8]
The German transgender association dgti e.V. opposed the Eunuch chapter in its response to the draft SOC8 — but with a revealing justification: “The medical treatment recommendations resemble those for non-binary persons and can be merged with them.”[9] The dgti thereby confirms it itself: the procedures are the same. The label is to disappear. The content is to be continued under “non-binary”.
In German Reddit communities, the boundaries have long since blurred. In forums such as r/nullectomy, r/germantrans and relevant eunuch communities, the same German clinics are recommended, the same surgeons discussed, the same cost estimates shared. Non-binary and eunuch-identified individuals share the same infrastructure — because they are seeking the same procedures.[10]
Hormones — permanent, visible, consequential
Surgical procedures are only the visible part. What often goes unmentioned: gender-affirming interventions almost always begin with hormonal measures — and for many, they never end there.
WPATH SOC8 recommends the same hormonal measures for “non-binary” persons as for “binary transsexuals”: testosterone for females, oestrogen and anti-androgens for males. For minors, puberty blockers are additionally recommended — GnRH agonists such as leuprorelin acetate or triptorelin, which suppress the body’s natural pubertal development.
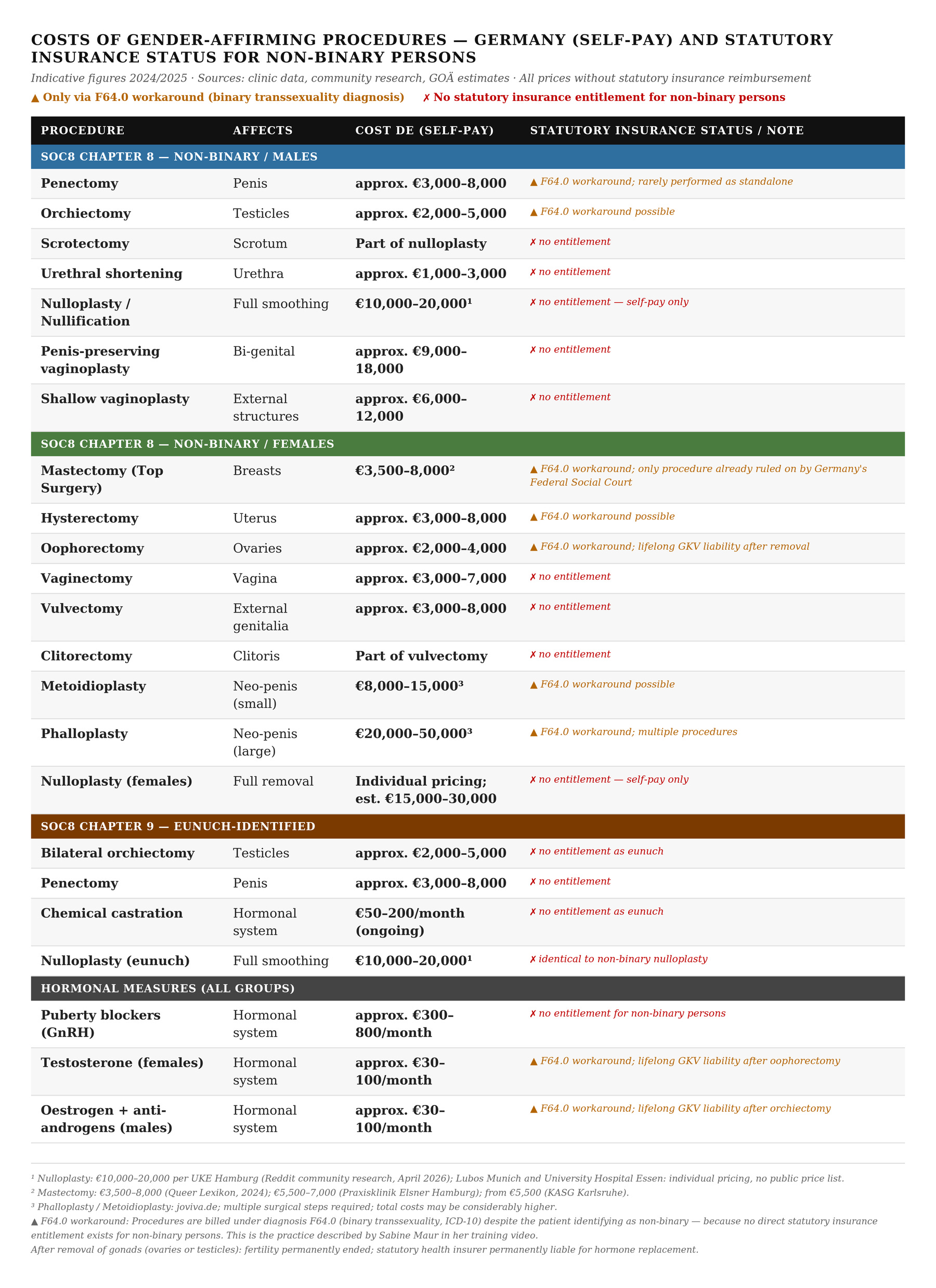
In Germany, some of these hormones are already covered by statutory health insurance under the diagnosis F64.0 (binary transsexuality, ICD-10). For non-binary persons, there is currently no formal entitlement — the F64.0 workaround is used in practice.
The long-term medical consequences are considerable and inadequately documented in the clinical literature:
Puberty blockers do not merely suppress puberty — they also suppress bone density development and brain maturation. When not discontinued, they lead to subsequent hormone therapy in almost all those affected — a transition that is rarely reversed in practice.[11]
Testosterone in girls and women causes visible, sometimes irreversible changes: voice deepening, clitoral enlargement, facial hair, androgenic hair loss. Systemic long-term effects include elevated cardiovascular risk and atrophy of the uterus and ovaries.
Once an oophorectomy (removal of the ovaries) is performed, endogenous oestrogen production ceases permanently. The woman is dependent on lifelong hormone replacement.
Orchiectomy in males (removal of the testicles) permanently ends testosterone production. Here too, lifelong hormone replacement is the consequence.
This has profound implications for the statutory health insurance system: once the gonads are removed, the GKV is permanently liable. The one-off cost of the operation is only the beginning. Lifelong ongoing costs follow: hormone replacement, bone density monitoring, cardiovascular monitoring, cancer screening for removed organs. Once ovaries or testicles are removed, fertility is irreversibly ended.
None of these follow-on costs are addressed in Minister Warken’s G-BA mandate.[12]
For clarity: not everyone who identifies as non-binary wishes to undergo all of these procedures. But it should be clear that “non-binary” functions as a gateway to any desired procedure — however drastic. The goal is for health insurers to fund all of these interventions.
Nulloplasty in Germany — “Think of a Barbie”
Until now it was unclear whether nulloplasties were being performed in Germany. German clinics do not advertise — as their US counterparts do — with this drastic form of body modification. However, it has already been anticipated in the German guidelines on transgender surgery.
Research in German-language Reddit communities now reveals that these procedures are already possible in Germany.
Reddit communities focused on these procedures — including r/germantrans, r/nullectomy and r/bodymods — describe the procedure as follows:
“Nulloplasty/Nullectomy leaves everything flat except the urethra. Think of a Barbie.”
These are active, publicly accessible forums in which German clinics, surgeons, waiting times and insurance coverage questions are discussed. Users help each other to access the procedures.
An extensive research compilation shared on r/nullectomy lists specific German clinics that offer or have performed nulloplasties:[13]
UKE Hamburg: nulloplasty possible, not yet performed; cost without insurance: €10,000–20,000
University Hospital Essen: already performed; earliest first consultation January 2027
Lubos Clinics Munich: already performed; considered highly experienced by the community
University Hospital Munich: can be performed
Klinik Sans Souci, Potsdam: can be performed; psychological assessment only to exclude organic brain disorders — no trans or non-binary documentation required
Itzehoe Hospital: can be performed
At the end of the compilation, one telling sentence stands out:
“A very important problem in Germany, though: Apparently nothing related to non-binary gets covered by any health insurance. I am currently in the process of trying to find ways around this.”
The procedures are already a reality. What is missing is the insurance funding.
The F64.0 workaround
For statutory health insurance reimbursement, the diagnosis F64.0 — binary transsexuality under ICD-10 — is currently required. For persons who identify as non-binary, this route is officially closed. The workaround is well known in the community:
“If the clinic goes along with it, it would just pass as a standard gender-affirming procedure.”
Non-binary patients are simply billed under F64.0 — because there is no other route to insurance funding. This is precisely what Maur explained in her training video.[14]
Warken’s G-BA mandate is intended to make this workaround unnecessary: a dedicated reimbursement basis for non-binary persons is to be written directly into the ambulatory specialist care (ASV) guideline — without an evidence assessment procedure, without parliamentary approval.
“Gender incongruence” in ICD-11: no longer a disease — yet still to be funded by statutory insurance
The timing of this pressure is not coincidental — it has a specific legal background. Germany is in the transition phase to ICD-11, the WHO’s new international classification of diseases. Under ICD-10, “transsexualism” is classified as a mental disorder — this is the legal basis on which GKV benefits are currently approved. Under ICD-11, the category is renamed “gender incongruence” and is explicitly no longer classified as a mental disorder.[15]
This may sound like progress — but it has a legally explosive consequence: if gender incongruence is no longer a disease, the existing legal basis for insurance funding falls away. The Federal Social Court made this explicit in its 2023 ruling: the statutory health insurance system does not recognise an entitlement to body-modifying treatments that exists independently of the presence of a medical condition.[16] Without a separate statutory basis — comparable to §27a SGB V for artificial insemination — the insurer does not pay.
This is the real explosive power of the ICD-11 transition for Germany: those who push forward the destigmatisation agenda — “not a mental illness!” — simultaneously remove the existing legal basis for insurance funding. Warken’s G-BA mandate is an attempt to close this gap before it becomes visible in public discourse.
Surgeon and guideline author in one person
The Reddit community explicitly recommends Prof. Dr. Jochen Heß at the University Hospital Essen for nulloplasties — the hospital confirms that such procedures have already been performed there. Heß is simultaneously a co-author of the German guideline for surgical interventions in gender incongruence (AWMF S2k, June 2025).[17]
A surgeon who performs nulloplasties is co-authoring the guideline that is intended to turn these procedures into covered health insurance services.
This guideline explicitly names WPATH SOC8 as its authoritative international reference. Nulloplasty does not appear in the guideline by name — but it describes procedures in which all primary and secondary sex characteristics are removed in one or two stages. In other words: what WPATH defines as Nulloplasty is present in the German guideline — just under a different name.
How “non-binary” is supposed to enter the GKV — and why this does not hold up
The letter of instruction dated 28 January 2026 makes unmistakably clear how Warken intends to direct the G-BA. She explicitly writes that the G-BA should determine the scope of treatment “without this necessarily requiring a complex and time-consuming benefit assessment procedure.”[18]
Yet the benefit assessment procedure under §135 SGB V is precisely what the Federal Social Court identified as the competent procedure in its October 2023 ruling. The case was brought by a person who identified as non-binary and had paid for a bilateral mastectomy out of pocket — €5,305.32 — claiming reimbursement from the Techniker Krankenkasse. The BSG dismissed the claim: mastectomy for the treatment of gender incongruence constitutes a new treatment method within the meaning of §135 SGB V and may only be reimbursed after a benefit assessment by the G-BA.[19]
In doing so, the court passed the ball directly to the G-BA — and explicitly stated that it was now the G-BA’s responsibility to assess the method and regulate the provision of care. Warken has picked up that ball — and is now circumventing precisely the procedure the court had in mind.
The reason is plain: the procedure would fail. The guideline on which the G-BA is to rely — WPATH SOC8 — actively suppressed its own evidence base.
In 2018, WPATH commissioned the Evidence-Based Practice Centre at Johns Hopkins University to carry out a systematic evidence review. The result: little to no evidence for the benefit of hormonal and surgical interventions in children and young people. WPATH never published these findings — and forced Hopkins to withdraw completed manuscripts. This is documented in unsealed court records from a 2024 US federal case.[20]
The German AWMF guideline, which is intended to serve as the basis for the G-BA, consequently had to be downgraded from an evidence-based guideline to a mere consensus guideline — because the studies were lacking.[21]
WPATH buried the evidence review because the findings would have jeopardised insurance funding. Warken is bypassing the assessment procedure because it would lead to the same result.
Vulnerable girls — the intended target group
The term “non-binary” did not enter German law through the front door. On 10 June 2021, the Child and Youth Strengthening Act (KJSG) came into force, amending §9 SGB VIII: providers of child and youth welfare services are now required to “take into account the different life situations of girls, boys, and transgender, non-binary and intersex young people.”[22] This was the first mention of “non-binary” in any German federal statute — introduced in the context of anti-discrimination, without the category being defined.
The Self-Determination Act (SBGG), in force since 1 November 2024, enshrined “diverse” as a personal status option — again without defining what “non-binary” or “diverse” means.[23] A declaration to the registry office suffices.
If a GKV guideline is to establish entitlements for “non-binary persons”, it will apply to a group that the law has nowhere described.
The data shed light on who this group actually is. According to an analysis of nationwide GKV data (Bachmann et al., Deutsches Ärzteblatt 2024), female adolescents aged 15 to 19 have shown the sharpest rise: from 38 per 100,000 in 2013 to 452 per 100,000 in 2022 — a twelvefold increase in ten years.[24] A representative study of over 122,000 young people in Wales found that 80% of gender-minority adolescents were female. Non-binary young people showed the highest rates of emotional difficulties and behavioural problems — higher than those identifying as transgender.[25] Clinical studies consistently show that girls and young women presenting at gender clinics frequently have backgrounds involving trauma, eating disorders, ADHD, autism and self-harm.[26]
A concrete case illustrates what this means in practice. The Queer Lexikon operates a publicly accessible “problem page” (“Kummerkasten”) explicitly aimed at children and young people, funded with public money.[27] In response Nr. 4,456 of 5 February 2024, a girl or young woman who identifies as a trans man writes:
“I am trans male and will soon get blockers and hopefully then in the coming years testosterone, I am happy with all my decisions and am also desperately waiting for the mastectomy. […] I feel extreme dysphoria about my genitals and would really love an operation that changes that, but I also can’t really imagine having a penis. […] I would most like to have absolutely nothing there, to feel nothing etc.”
The fact that she is still waiting for puberty blockers, with testosterone and a mastectomy still ahead of her, strongly suggests she is a minor in an early stage of medical transition.
The response from “Elias” of the Queer Lexikon team recommends Nulloplasty — and explains that this procedure is available “only in the USA so far”. This was factually incorrect at the time of publication in February 2024: Lubos Clinics Munich had already performed nulloplasties, UKE Hamburg declared the procedure possible, and the University Hospital Essen was likewise performing it.
What Elias recommended to this girl is the complete operative removal of all female genital structures: uterus, ovaries, vagina, clitoris, labia. An irreversible procedure that permanently ends fertility and eliminates all erogenous zones. Recommended in a publicly funded problem page for minors, to a girl who says she wants “absolutely nothing” there anymore.
That minors will be affected by the G-BA guideline was acknowledged by Warken herself in her letter of instruction: the regulation would include “precisely those special features that need to be observed for the protection and evidence-based care of affected children and young people.”[28] A promise that is legally unenforceable given the absence of any definition of the target group.
What this all means
The term “non-binary” sounds harmless. Hardly anyone can form a precise idea of what it means.
Yet what has been smuggled into German law under the cover of this term — and is now intended to become a statutory health insurance benefit — is anything but harmless: even extreme, body-damaging measures, manipulations of the hormonal system and plastic surgery on the genitals are to be funded on demand by the general public. And a single procedure is rarely the end of it: the deliberate destruction of the endocrine system and the removal of the gonads generate permanent ongoing costs.
Nulloplasty is one of the most extreme forms of plastic surgery and severe physical harm. One could hardly convince the public to fund the castration of men who identify as eunuchs. With the labels “non-binary” and “Nulloplasty”, hardly anyone asks what exactly is meant.
WPATH guidelines are regularly presented in the debate as instruments of protection. The Kiefel case shows what this looks like in practice: the providers considered the SOC8 too restrictive and actively circumvented them. Brave Space and Amy Ruff, according to the lawsuit, rejected the WPATH standards as too high a barrier and replaced them with a system of maximum accessibility. What is supposed to function as a minimum standard becomes an option. The patient’s wish takes precedence.
In a recent interview, Sabine Maur describes something similar as her ideal: less gatekeeping, more trust in patients and practitioners — and ICD-11 explicitly as an instrument for securing GKV funding.[29] Non-binary persons had, she says, been “simply excluded” — yet they make up “no less than 30 to 40% of the trans community”. Her model: maximum patient self-determination, minimal barriers for practitioners, costs borne by the general public. The provision of care for non-binary persons is, in her view, to be transferred from the self-pay sector into statutory insurance coverage — by precisely the route that Warken’s G-BA mandate is currently pursuing.
In view of the sweeping austerity measures in the healthcare system, and above all in order to protect vulnerable girls and young women, Nina Warken, the G-BA and the GKV should refrain from funding these drastic, experimental procedures. As with the proceedings that Sabine Maur has brought against me: the goal is to bring into public view what transgender interventions actually mean — and how the actors who promote them are going about it.
[1] Camille Kiefel v. Amy Ruff / Brave Space and Mara Burmeister / Quest Center for Integrative Health, Circuit Court Multnomah County, Oregon. Confidential settlement January 2026; Kiefel had sought $3.5 million. First report: Benjamin Ryan, “Detransitioner Settles Malpractice Lawsuit Days Before Trial In Oregon”, Hazard Ratio / Substack (29.04.2026). benryan.substack.com
[2] Fox Varian v. Kenneth Einhorn / Simon Chin, Westchester County Supreme Court, New York, verdict 30.01.2026. Washington Times (02.02.2026). washingtontimes.com
[3] Federal Trade Commission et al. v. World Professional Association for Transgender Health, U.S. District Court for the Northern District of Texas, filed 17.06.2026. FTC press release: ftc.gov
[4] GKV-Spitzenverband, Circular 2026/070 of 03.02.2026, enclosure: letter from Federal Health Minister Nina Warken to G-BA Chair Prof. Josef Hecken of 28.01.2026; BMG reference 40227#00002 (30.01.2026). Via FragDenStaat: fragdenstaat.de — BSG, judgment of 19.10.2023, B 1 KR 16/22 R: bsg.bund.de
[5] WPATH, Standards of Care for the Health of Transgender and Gender Diverse People, Version 8 (SOC8), September 2022, Chapter 8 “Non-binary” (p. 80 ff.) and Chapter 9 “Eunuchs” (p. 88 ff.). doi.org/10.1080/26895269.2022.2100644
[6] QueerDoc, “Nullectomy/Nullification” (2022/2023). queerdoc.com/nullification-nulloplasty
[7] QueerDoc, “Nullectomy/Nullification” (2022/2023). queerdoc.com/nullification-nulloplasty
[8] Genevieve Gluck / Reduxx, “Top Trans Medical Association Collaborated With Castration, Child Abuse Fetishists” (May 2022). reduxx.info — Also: “Academics Involved With Top Transgender Health Authority Publish Paper on ‘Choosing Castration’” (19.11.2022). reduxx.info
[9] DGTI e.V., “Commentary on the draft Standards of Care V8 (SoC V8) of WPATH” (23.01.2022). dgti.org
[10] Reddit r/nullectomy, German clinic compilation (April 2026). No permalink; archived by the author.
[11] Cass Review, Final Report (April 2024): “No evidence that puberty blockers buy time to think; most youth on them proceed to cross-sex hormones.” cass.independent-review.uk
[12] Letter from Federal Health Minister Nina Warken to Prof. Josef Hecken (G-BA) of 28.01.2026; BMG accompanying letter to GKV-Spitzenverband, reference 40227#00002 (30.01.2026). Published as enclosure to GKV Circular 2026/070 of 03.02.2026. fragdenstaat.de
[13] Reddit r/nullectomy, German clinic compilation (April 2026). No permalink; archived by the author.

[15] WHO, ICD-11, Chapter 17 (Conditions related to sexual health), HA60 “Gender incongruence of adolescence or adulthood”. icd.who.int
[16] Federal Social Court (BSG), judgment of 19.10.2023, B 1 KR 16/22 R. bsg.bund.de
[17] AWMF S2k guideline “Surgical measures in gender incongruence”, Reg. No. 043-052, June 2025. register.awmf.org
[18] Letter from Federal Health Minister Nina Warken to Prof. Josef Hecken (G-BA) of 28.01.2026; BMG reference 40227#00002 (30.01.2026). fragdenstaat.de
[19] Federal Social Court (BSG), judgment of 19.10.2023, B 1 KR 16/22 R. bsg.bund.de
[20] Unsealed court documents from Boe v. Marshall, U.S. District Court, Middle District of Alabama, Case No. 2:22-cv-00184, unsealed June 2024. Expert Report James Cantor Ph.D. Summary: Jesse Singal (25.06.2024). jessesingal.substack.com — Mia Hughes / Environmental Progress, “The WPATH Files” (March 2024). environmentalprogress.org
[21] AWMF S2k guideline “Surgical measures in gender incongruence”, Reg. No. 043-052, June 2025. register.awmf.org
[22] Child and Youth Strengthening Act (KJSG) of 03.06.2021 (BGBl. I p. 1444). §9 SGB VIII: gesetze-im-internet.de
[23] Act on Self-Determination Regarding Gender Entry (SBGG) of 12.04.2024 (BGBl. I No. 122), in force from 01.11.2024. gesetze-im-internet.de
[24] Bachmann CJ, Golub Y, Holstiege J, Hoffmann F: “Gender identity disorders among young people in Germany: prevalence and trends, 2013–2022.” Deutsches Ärzteblatt International 2024; 121: 370–1. doi.org/10.3238/arztebl.m2024.0098
[25] Study of 122,766 young people in Wales (aged 11–16): “Emotional and behavioural difficulties in gender minority compared to cisgender adolescents.” PMC, 2025. pmc.ncbi.nlm.nih.gov
[26] Cass Review (2024): Documents complex psychiatric comorbidities, neurodevelopmental disorders and adverse childhood experiences as the norm in the clinical population. Finnish registry studies: nearly half of over 2,000 adolescents had received psychiatric treatment prior to referral to a gender clinic. cass.independent-review.uk
[27] Queer Lexikon, problem page response No. 4,456 (05.02.2024). queer-lexikon.net — Public funding documented: Apollo News (04.05.2024). apollo-news.net
[28] Letter from Federal Health Minister Nina Warken to Prof. Josef Hecken (G-BA) of 28.01.2026. fragdenstaat.de
[29] Sabine Maur in Bonner Duett: “Wie verbessern wir Psychotherapie und Trans-Gesundheit?”, YouTube, archived 16.06.2026. youtube.com/watch?v=E5T3nZVw0OQ — Relevant timestamps: approx. 00:57 (ICD-11 as instrument of cost reimbursement), approx. 00:59 (non-binary persons “simply excluded” — 30–40% of the trans community), approx. 01:21 (trust in patients and practitioners as guiding principle).