
Non-binary — Undefined, Unproven, at Public Expense
How German Health Minister Warken Bypasses Parliament — and What the Sabine Maur Case Reveals


1. A Video, a Confession, a Resignation
On 23 March 2026, Sabine Maur resigned as Vice President of the Federal Chamber of Psychotherapists (BPtK) and as President of the Rhineland-Palatinate Chamber of Psychotherapists.[1][2] The occasion was, among other things, a leaked video from a professional training seminar for psychotherapists, in which Maur recommends the following: when patients identify themselves as “non-binary,” therapists should conceal this fact from the health insurer — because “non-binary” is regularly treated by insurers as grounds for exclusion. She referred to the current legal situation as “absurd ethical conflicts.”[3]
Maur, one of the lead authors of Germany’s official treatment guideline for children and adolescents with so-called “gender incongruence,” thus knew that the statutory right to reimbursement for so-called non-binary persons does not currently exist under law.
Maur had attempted to use an application for a preliminary injunction against me to bring the critical public discussion of her conduct and the video’s circulation to a halt through the courts. She refused a settlement, demanded a judgment, and lost before the Berlin District Court on the main points (the proceedings have been documented in full on the Frauenheldinnen website and on my Substack).[4] The video has become a document of contemporary history.
What this reveals is a system that is aware that its own foundations do not hold and that seeks to suppress this knowledge at all costs. At the same time, certain temporal parallels are worth noting.
On 28 January 2026, Federal Health Minister Nina Warken had quietly, and without any parliamentary debate, commissioned the Federal Joint Committee (G-BA) to establish as a statutory health insurance benefit precisely those care structures that Maur herself had treated as lacking legal coverage.[5][6] The timing is remarkable: Maur’s cease-and-desist notice against me had arrived two days earlier. Subsequently, the newspaper Die Welt had also reported on the matter and was threatened with legal action.[7] It appears that public critical debate was to be prevented.
This is consistent with the fact that various organizations[8] are now attempting to portray the ruling against Maur as an anti-trans campaign and use it as political leverage. The argument runs: the judgment has made clear that non-binary patients are in practice excluded from the reimbursement system — so the political system must finally create a regulatory framework. Maur is portrayed as a victim, even though she herself initiated the proceedings, refused a settlement, and received a judgment certifying that her conduct violated professional law.
The ruling that holds Maur accountable for her conduct is thus invoked as the justification for precisely the political demand that made Maur’s conduct necessary in the first place. Evidently, these developments would have been preferred to proceed away from public scrutiny. That calculation was thoroughly foiled by my refusal to sign the cease-and-desist notice.
This article explains how all of this has been possible, why it is unlawful, and why women and girls are directly affected.
2. What “non-binary” is — and what it is not
What exactly is a “non-binary gender identity”? The honest answer is: a self-identification without biological, neurological, or genetic basis.
2.1 The Academic-Activist Origins of the Term
The term originates in US queer activism of the early 1990s. The activist Riki Anne Wilchins coined the precursor term “genderqueer” in 1995 in the newsletter of the Transsexual Menace as a political umbrella term — explicitly for transvestites, cross-dressers, transsexuals, and all those who subvert gender norms.[9] The actual term “non-binary” only appeared around the year 2000 and spread widely only in the early 2010s via social media.[10] Judith Butler provided an academic theory of gender-as-performance in Gender Trouble (1990), but was not the origin of the term and only publicly identified as non-binary in 2019.
2.2 Absence of Scientific Foundation
What is the scientific basis for this category? There is none. All mammals, including humans, are organized into two sexes in terms of reproductive biology. The known variations in sex development (so-called Differences of Sex Development / DSDs, colloquially referred to as “intersex”) are rare developmental deviations, not a third sex. There is no biomarker, no brain anatomy, no genetic signature for a “non-binary gender identity.”
The American Psychological Association (APA) itself acknowledges that the empirical research base for non-binary identities is inadequate.[11] The British Cass Report (2024) finds that the rise in discomfort with one’s own body and sex (”gender dysphoria”) among young people is explicable through psychosocial factors, not biological ones.[12] The AWMF’s 2025 children’s and adolescents’ guideline could not even attain the status of an evidence-based S3 guideline due to a lack of controlled efficacy studies — it was downgraded to the lower S2k level (purely consensus-based) and remains contested.[13]
“Non-binary” is therefore not a medical diagnosis. It is a self-description that emerged within a specific cultural and academic tradition in the English-speaking world of the 1990s.
3. The Circular Logic: How Identity Politics Became a Public Health Insurance Benefit
If “non-binary” has no scientific basis, how has this category entered German treatment guidelines and, ultimately, jurisprudence?
The answer is a mechanism that may be described as an epistemic circle. Each stage confers legitimacy upon the previous one, without any independent external evidence assessment according to the standards of evidence-based medicine occurring at any point.
The roots of this circle extend back to the 1970s, when WPATH (World Professional Association for Transgender Health) was still operating under the name Harry Benjamin International Gender Dysphoria Association. Even then, the category of transsexualism was not based on biological findings but on self-report, though at least institutional thresholds existed. These were dismantled step by step on grounds of discrimination. The end point is complete self-diagnosis and self-directed treatment.
The individual steps:
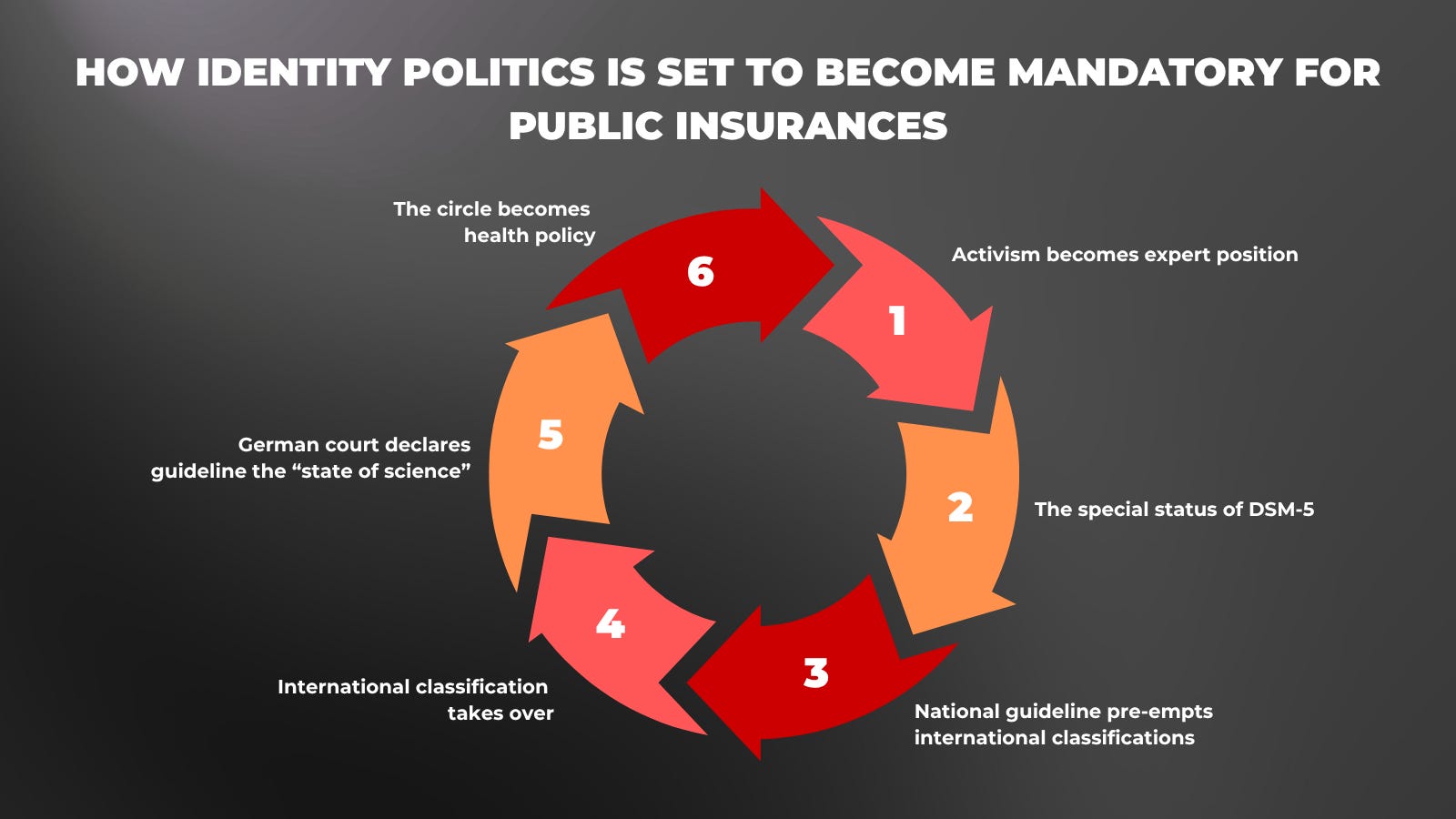
Step 1 — Activism becomes expert position
Since the 1970s, internationally activist-oriented organizations such as WPATH have produced treatment guidelines — the “Standards of Care” (SOC). WPATH’s SOC-7 (2012) mentions gender-nonconforming persons but still contains no dedicated chapter on non-binary identities. The SOC documents rest on expert consensus in which activists were involved. No independent external evidence assessment took place. The Cass Review (2024) explicitly assessed SOC-8 as a guideline lacking “developmental rigour and transparency.”[14]
Step 2 — The special status of DSM-5
The diagnosis “gender dysphoria” in the DSM-5 (2013) is the only psychiatric diagnosis in which the patient essentially establishes the diagnosis themselves, determines the desired treatment themselves, and where this treatment leads to irreversible physical interventions. Neither anorexia nor Body Dysmorphic Disorder uses the patient’s treatment wish as the basis for treatment. The working group that developed this diagnosis was personnel-linked to the WPATH network.[15]
Step 3 — National guideline pre-empts international classifications
The AWMF S3 guideline for adults (October 2018) explicitly references ICD-11 and DSM-5 and expressly includes non-binary persons as treatment-seekers, even though ICD-11 had not yet been adopted (it followed in May 2019) and WPATH had no dedicated non-binary chapter (SOC-8, 2022). The evidence base comes from the same research network as the guideline itself. The evidence is predominantly Grade III, the lowest evidence grade in the AWMF system. The S3 guideline for adults expired in October 2023 and has been officially invalid since then. A new S3 for adults is not expected until 2027.[16]
Step 4 — International classification takes over
The WHO adopts ICD-11 (May 2019, in force since January 2022) with the category “gender incongruence” (HA60), de-pathologizes it, and expressly includes non-binary identities. WPATH follows in 2022 with SOC-8, which for the first time contains a dedicated chapter on non-binary persons — simultaneously with a chapter on so-called eunuchs, without a biological basis for either category.
The trans lobby organization dgti e.V. called in its commentary on the SOC-8 draft for the eunuch chapter to be merged with the non-binary chapter, on the grounds that the medical treatment recommendations were equivalent. This would mean: interventions aimed at the complete removal of primary sex characteristics would be classified as a non-binary benefit entitlement.[17]
Crucial for the German legal situation: ICD-11 has not been introduced into social law in Germany to this day. The statutory health insurance system (GKV) continues to operate on the basis of ICD-10, code F64.0 — a code that covers only binary transsexualism.[18]
Step 5 — German court declares guideline the “state of science”
The Federal Social Court (FSC) writes in its judgment of 19 October 2023: “The state of scientific knowledge as reflected in the current S3 guideline explicitly encompasses non-binary gender incongruences as well.” The Court equates the guideline with science, even though the relevant guideline had already expired and its evidence base corresponded predominantly to Grade III. Crucial: the FSC did not thereby establish a reimbursement obligation for non-binary persons. It referred the question to the parliamentary legislature — not to the Minister.[19]
Step 6 — The circle becomes health policy
Warken commissions the G-BA on 28 January 2026 to develop a statutory health insurance reimbursement guideline — deliberately circumventing the benefit assessment procedure under Section 135, which the FSC ruling designated as the applicable procedure. The FSC has made unmistakably clear that the legal basis is to be created above all by the parliamentary legislature. Without this parliamentary step, the G-BA cannot issue a legally sound guideline — it would be building on sand.[20]
The legislative path into German law
The medical circle does not run alone. In parallel, “non-binary” was introduced into German law through the legislative route — consistently without definition.
In the Social Code Book VIII (SGB VIII), the term “non-binary” first appeared in the statutory text in 2021, in the context of the promotion of socially disadvantaged children and young people.
A ruling of the Federal Constitutional Court of 10 October 2017 (1 BvR 2019/16) obliged the legislature to create a third option in civil status law, intended exclusively for persons with documented disorders of sex development. The provision was subverted by trans activists for changes of civil status without verification.[21]
With the Self-Determination Act of 1 November 2024, even this prerequisite was abolished. A simple self-declaration now suffices.
In none of these laws is “non-binary” defined. What appears in civil status law serves in the next step as the argument for statutory health insurance entitlements. This is how the legislative and medical pathways converge.
At the end of these chains lie unlimited elective interventions to be financed by the general public through the health insurance funds — for a category that rests on self-report and whose existence has never been scientifically demonstrated. In the United States, interventions for so-called “non-binary” individuals culminate in so-called nullification surgeries,[22] in which all primary and secondary sex characteristics are removed.
Sabine Maur knows these circles. That is why she recommended in her video that the insurer side be deceived: she knew that the circular loop had not yet been closed at precisely this point — in the law on reimbursement. The Federal Social Court had torn it apart in October 2023.
4. The FSC Ruling 2023: What It Actually Says
The judgment of the Federal Social Court (FSC) of 19 October 2023 (B 1 KR 16/22 R) is described by trans organizations and gender-affirmative physicians and therapists as an unfavorable ruling that urgently needs to be corrected. However, the Court established something fundamental that calls into question the entire prior practice of Germany’s statutory health insurance funds.
4.1 New Methods Require Federal Joint Committee Approval
The Court held: gender-affirming surgeries are new methods of examination and treatment within the meaning of Section 135 para. 1 SGB V.[23] This means: the so-called “prohibition with authorization reservation” applies.[24] A new method may only be provided at the expense of the statutory health insurance system once the G-BA has expressly recommended it — following a benefit assessment and review of medical necessity and cost-effectiveness.
This recommendation is entirely absent. Since its establishment in 2004, the G-BA had never fundamentally examined so-called “transition treatments.” The previous GKV reimbursement had no statutory basis.
4.2 The Parliamentary Legislature Must Act
The FSC further writes that the creation of a legal basis “rests first and foremost with the parliamentary legislature,”[25] because the matter lies at the boundary between illness within the meaning of statutory health insurance and the constitutionally protected right to personal identity. This constitutes a direct call upon the Bundestag — not upon the Health Minister.
G-BA Chairman Josef Hecken understood this. He wrote to the Federal Ministry of Health on multiple occasions, most recently on 3 December 2024:[26] a benefit assessment procedure under Section 135 “would be uncertain given the high methodological requirements based on the current state of medical knowledge.” Even more plainly: “The current evidence base is inadequate with respect to the majority of measures specifically aimed at alleviating existing or preventing threatened gender dysphoria.”
Hecken had already acknowledged in June 2024 to the newspaper Tagesspiegel: in the event of a benefit assessment, “the evidence base would not have been sufficient to demonstrate a positive benefit for the various measures.” Had the procedure returned a negative result, “the insurers would have generally been prohibited from reimbursing the treatments, even if they had wanted to.”[27]
Hecken therefore pressed for a special statutory provision: a new Section 27c SGB V.[28] Such a provision would have had to be debated and passed by parliament. That has not happened.
The National Association of Statutory Health Insurance Funds (GKV-Spitzenverband) had meanwhile made clear: until a new statutory regulation is in place, “an extension of eligibility to non-binary persons is not possible.”[29][30]
5. Warken’s Trick: Section 116b Instead of Section 135
Nina Warken did not make the statutory amendment to SGB V. Instead, on 28 January 2026, she directly commissioned the G-BA[31] — not via Section 135, i.e., not via the benefit assessment procedure that the FSC ruling requires — but via Section 116b SGB V, the provision governing specialized outpatient medical care (ASV).
In her commission, Warken explicitly writes that no benefit assessment procedure is required, as it would be “too complex and time-consuming.”[32] Instead, the G-BA should “determine the scope of diagnostic and therapeutic treatment.”
The commission was not mentioned with a single word in the G-BA’s annual press conference of 20 January 2026 — nine days before the commissioning letter.[33] Only in late March 2026, when the newspaper Tagesspiegel reported on it, was the public informed at all.[34] The G-BA began its work on 19 March 2026 and has one year.[35]
Warken acts as though she is implementing the Federal Social Court’s mandate. But the Court had demanded precisely the opposite: it declared the Bundestag to be competent — not the Ministry. The following three points establish why her approach is unlawful.
5.1 Three Breaches of Law
First: Direct contradiction of the FSC ruling.
The Federal Social Court explicitly classified “transition treatments” as new methods under Section 135 para. 1 SGB V.[36] Warken instructs the G-BA to bypass precisely the procedure that the highest social court has designated as necessary. The G-BA’s own information sheet states: new methods are reimbursable only once the G-BA has expressly recognized their benefit, medical necessity, and cost-effectiveness.[37] A G-BA guideline produced in this way is legally challengeable.
Second: Missing legal basis for “non-binary.”
Section 116b para. 1 sentence 2 no. 2 letter i SGB V lists “transsexualism” as a reimbursable condition — referencing ICD-10 code F64.0, the binary picture of transsexualism.[38] Non-binary identities are not listed in this catalogue. The commission to include “further treatment-requiring forms of gender incongruence” has no express statutory basis in Section 116b.
Third: Missing democratic legitimacy.
The 2025 coalition agreement contains no mention of GKV reimbursement for “transition treatments.”[39] Warken acts without a parliamentary mandate, without public debate, and without transparency. Through an administrative commission to a subordinate self-governing body, she creates entitlements to benefits for which the highest social court has demanded a parliamentary regulation.
6. What Is at Stake
This debate is typically framed as if it concerned exclusively the persons seeking treatment. That framing is, however, too narrow. The planned G-BA guideline touches on several questions of fundamental societal and women’s rights significance.
6.1 Solidarity Community and Resource Allocation
The GKV is a solidarity community. Benefits financed from it must demonstrate utility, medical necessity, and cost-effectiveness. This protects all insured persons, including women who depend on these funds for reproductive health care, contraception, childbirth, and gynaecological treatment. Hormonal and surgical interventions without an evidence base, for a category without a biological correlate, burden this community.
6.2 Protection of Girls and Young Women
The rise in diagnoses of so-called “gender dysphoria” — i.e., distress about one’s own body and sex — disproportionately affects girls and young women. Recent studies show that in the majority of cases, the wish to belong to the other sex no longer persists in adulthood.[40][41] Irreversible interventions — mastectomy, hysterectomy, hormone treatment — in minors or young adults who may grow out of their bodily distress is a question of protecting the physical integrity of girls.
6.3 Women as a Category
A health care system founded on the principle that sex is pure self-definition has consequences for sex-specific statistics, sex-specific health care services, and access to women’s spaces and facilities. The decoupling of biological sex from the legal sex entry makes it increasingly difficult to collect sex-specific data and to use it as a basis for protecting women.
6.4 The Feminist Objection: Non-binary Does Not Solve the Underlying Problem
The original feminist position is this: biological sex should not determine what forms of expression, interests, occupations, or opportunities a person has. That is the core of the feminist liberation struggle: not the abolition of the concept of sex, but liberation from sex-role stereotypes (”gender”).
Being a woman does not mean one must be feminine, wear skirts, or enjoy domestic work. Being a man does not mean one is not allowed to show emotions or choose caring professions. If this fundamental insight is consistently pursued, the large majority of the histories of suffering behind the label “non-binary” dissolve. Body modification is not the solution — rather, reconciliation with one’s own body and societal change in favor of girls and women.
The “non-binary” label offers a false solution grounded in an unrealistic worldview that glorifies body-altering interventions. Women are made permanently dependent on interventions rather than having their autonomy and self-confidence strengthened.
6.5 The Finnish Register Study 2026: Psychiatric Burden Increases Post-Transition
A Finnish register study published in April 2026 in Acta Paediatrica, involving 2,083 affected individuals and 16,643 matched controls, directly contradicts the central promise of gender-affirmative care. Psychiatric morbidity rose from 45.7% before to 61.7% after first clinical consultation — while the control group remained stable at 14.6%. The authors conclude: severe psychiatric disorders do not decrease after medical transition; in some cases, deterioration is observed.[42]
For the G-BA decision, this is directly relevant: if the central reimbursement argument — that the treatment alleviates suffering — is not supported by the most comprehensive register study, that reimbursement justification collapses. Trans activists have criticized the study,[43] but even the critics cannot refute what Hecken has long acknowledged: the evidence does not suffice for a positive benefit assessment.[44]
6.6 Section 1631c BGB: The Ignored Prohibition on Sterilization
“Parents cannot consent to the sterilization of their child. The child itself cannot consent to sterilization either.” (Section 1631c German Civil Code / BGB)
This prohibition is absolute — regardless of the motive, regardless of whether sterilization is the primary goal or a side effect of treatment. A 2025 criminal law analysis by Woerner, Windsberger, and Roessner concludes: the standard combination of puberty blockers and cross-sex hormones leads with very high probability to permanent infertility — and could therefore fall under this absolute prohibition. Parental consent would then be invalid; treating physicians would risk criminal liability for bodily harm. A G-BA guideline recognizing such treatments as a statutory health insurance benefit cannot override Section 1631c BGB.[45]
7. The Connection That Exposes the System
In its 2023 ruling, the FSC relied on the S3 guideline for adults — a guideline that had already expired at that time. Warken’s commission invokes, in general terms, the “current state of medical knowledge.” Let us look at what that state of knowledge actually yields.
The S2k guideline for children and adolescents (AWMF 028-014, March 2025), in the development of which Sabine Maur participated as a representative of professional associations, expressly contains no recommendation for surgical interventions for non-binary minors and stipulates that puberty-blocking treatment is indicated only in very rare exceptional cases. The AWMF surgical guideline 043-052 (2025)[46] specifies no minimum age for body-modifying interventions and contains no specific recommendations for non-binary persons. Nonetheless, it describes the complete removal of all primary and secondary female sex characteristics in one- or two-stage operations — corresponding to the nullification surgeries recommended for non-binary persons in the United States.
There is a considerable gap between what the guidelines actually recommend and what activists demand. The S2k guideline for children and adolescents contains a dissenting opinion from three activist organizations calling for mastectomies in minors regardless of the binary character of their gender identity — contrary to the guideline’s actual recommendation.[47]
The influence of activist organizations extends into the official continuing education structure of the health care system: dgti e.V. — one of those organizations that intervened in the guideline process with dissenting opinions — has operated a quality circle for psychotherapists since 2023, whose meetings are certified by the Rhineland-Palatinate Chamber of Psychotherapists (LPK RLP). Sabine Maur was President of this Chamber until her resignation in March 2026. Each meeting awards three continuing education points, valid nationwide for the statutory training requirement. The certification costs are borne by the dgti itself.[48]
This is not science leading to policy. This is activism imitating science in order to become policy.
8. The Strategy Behind the System
The mechanism behind this is documented. In 2019, IGLYO (the international LGBTQI youth organization), the law firm Dentons, and the Thomson Reuters Foundation — the media and PR arm of the Thomson Reuters Corporation — jointly published a handbook for trans rights campaigns in Europe: “Only Adults? Good Practices in Legal Gender Recognition for Youth.” The document explicitly recommends:
avoiding public debate,
selectively targeting youth politicians,
using individual case studies for emotional persuasion, and
deploying “human rights” as a central campaign argument.[49]
Point 7 of the documented “Good Practices” demands state-funded treatment without the need for a diagnosis.
This precise strategy was applied in the passage of the Self-Determination Act. Broad parliamentary debate was prevented, the focus was placed on emotionally charged individual cases, self-determination of one’s sex register entry was declared a human right, and critics were aggressively silenced until the law was passed. Warken is now applying this same strategy to interventions that are not evidence-based: no public debate, no parliamentary mandate, the G-BA commissioned by ministerial letter.
“Human rights” is not a legally grounded claim here — it is campaign strategy. No international human rights treaty establishes a right to have others bear the costs of a self-definition and corresponding interventions. Human rights protect against state coercion. They do not obligate the insured community to finance irreversible physical interventions without an evidence base. It is not a human right to exit one’s biological sex at public expense.
The injunction proceedings that Sabine Maur brought against me have shown: the attempt to bring the public discussion about the video to a halt through the courts has failed. The silence spiral that the IGLYO handbook recommends as strategy has not worked in this case.[50]
Activists have undermined the guideline process with dissenting opinions. A major law firm and a media corporation have documented silence as strategy. Warken follows this strategy. And now the G-BA is to deliver what the science cannot deliver — at the expense of all insured persons, for a category that nobody has defined.
9. What Needs to Happen Now
The G-BA has until approximately March 2027 to develop its guideline.[51] Within the ASV guideline procedure, there will be a consultation and hearing process. This is a formal avenue for participation.
The decisive factor is political pressure on the Bundestag. The FSC explicitly established that the creation of a legal basis rests with the parliamentary legislature.[52] Warken has deliberately circumvented this path. Members of parliament — particularly on the Health and Legal Affairs Committees — should know that a minister is here creating statutory benefit entitlements by administrative commission, bypassing parliament, for entitlements that the highest social court has designated as lacking a statutory basis.
The following questions must be put publicly and answered in parliament:
On what precise statutory basis does Warken commission the G-BA to include non-binary status in the ASV guideline, when Section 116b para. 1 sentence 2 no. 2 letter i SGB V lists only transsexualism (F64.0)?
Why is the benefit assessment procedure under Section 135, designated by the FSC as the applicable procedure in its ruling, being bypassed?
Has the Bundestag consented to this commission, and if not: when will it be presented with it?
On what evidential basis is the G-BA to develop a guideline for treatments when the relevant guideline committee itself has acknowledged that it cannot make evidence-based recommendations?
Why was the G-BA commission not communicated at the G-BA annual press conference on 20 January 2026, and only became known following journalistic investigation in late March?
10. Conclusion
What is happening here is not a minor matter in the health bureaucracy. It is a case in which a minister creates a statutory benefit entitlement — by deliberately circumventing the benefit assessment procedure — that lacks parliamentary authorization, is legally contestable, and rests on an evidence base that its own authors could not defend.
Sabine Maur’s video is not the scandal — it is the revelation. It shows that those who built this system always knew where it does not hold.
The Berlin District Court rejected her attempt to suppress this knowledge.
It is time for the Bundestag to do the same.
Sources and References
Jurisprudence
FSC, judgment of 19.10.2023, B 1 KR 16/22 R — bsg.bund.de
FSC, judgment of 28.08.2024, B 1 KR 28/23 R (clarification on legitimate expectations)
Berlin District Court II, judgment March 2026, case no. 27 O 51/26 eV
Federal Constitutional Court, decision of 10.10.2017, 1 BvR 2019/16 (Third gender option in civil status law)
Documents (via Frag den Staat / FragDenStaat)
Letter from G-BA (Hecken) to Federal Ministry of Health, 29.11.2023
Letter from G-BA (Hecken) to Federal Ministry of Health, 03.12.2024 — Doc. 256809
Letter from Federal Ministry of Health (Lauterbach) to G-BA, 20.12.2024
GKV-Spitzenverband, circular 2024-063, 31.01.2024 — Doc. 245887
Commissioning letter from Federal Ministry of Health (Warken) to G-BA, 28.01.2026 — Doc. 1097939
GKV-Spitzenverband, circular 2025/102, 13.02.2025
Coalition agreement CDU/CSU/SPD 2025 — Doc. 258046
Guidelines (AWMF)
S3 Guideline 138-001: Gender Incongruence, Gender Dysphoria and Trans Health, October 2018 — valid until 08.10.2023, expired since then (register.awmf.org/de/leitlinien/detail/138-001)
S2k Guideline 028-014: Gender Incongruence and Gender Dysphoria in Children and Adolescents, March 2025
S2k Guideline 043-052: Surgical Measures for Gender Incongruence, June 2025
Press
N. Garrelts, Tagesspiegel Background, 24.03.2026: Health insurers and Warken at odds over hormone reimbursement
N. Garrelts, Tagesspiegel Background, 26.06.2024: Hecken sends regulatory proposal to Ministry
A. Kroening, Die Welt, 30.03.2026: “Absurd ethical conflicts,” a resignation
A. Kroening, Die Welt, 12.02.2026: “Absurd ethical conflicts” — and how the insurer is still supposed to pay
T. Amelung, QueerNations, 24.03.2026: After video leak and court ruling: Sabine Maur steps down
TTSB, 27.03.2026: GKV reimbursement: the G-BA is to cut the Gordian knot
Science
J. Butler, Gender Trouble: Feminism and the Subversion of Identity, Routledge, 1990
Cass Review, Final Report, NHS England, April 2024
P. Rawee et al., Development of Gender Non-contentedness During Adolescence and Early Adulthood, Archives of Sexual Behavior 53, 2024
U. Bachmann et al., Gender identity disorders in young people in Germany: frequency and trends 2013–2022, Dt. Aerzteblatt International 121, 2024
WPATH, Standards of Care Version 8, International Journal of Transgender Health 23(S1), 2022
WPATH, Standards of Care Version 7 (SOC-7), International Journal of Transgenderism 13(4), 2012
ICD-11 (WHO, adopted May 2019, in force January 2022), Code HA60: Gender Incongruence — icd.who.int
R. A. Wilchins, “In Your Face” (newsletter The Transsexual Menace), 1995
J. Haynes / J. McKenna (eds.), Unseen Genders: Beyond the Binaries, New York 2001
S. Monro / D. Crocetti et al., “Non-binary and genderqueer: An overview of the field”, International Journal of Transgenderism 20(2–3), 2019
S.-M. Ruuska, K. Tuisku, T. Holttinen, R. Kaltiala, “Psychiatric Morbidity Among Adolescents and Young Adults Who Contacted Specialised Gender Identity Services in Finland in 1996–2019”, Acta Paediatrica (2026), doi:10.1111/apa.70533
L. Woerner, A. Windsberger, V. Roessner, “Gender-affirming medical measures for minors as a violation of Section 1631c BGB? — A critical criminal law assessment”, ZfIStw 5/2025, pp. 1718ff.
Statutes and Norms
Section 116b SGB V — Specialized outpatient medical care
Section 135 para. 1 SGB V — Benefit assessment procedure
Section 27 para. 1 SGB V — Medical treatment
Self-Determination Act (SBGG), BGBl. I Nr. 206, 19.06.2024
Section 1631c BGB — Prohibition on sterilization of minors
SGB VIII Section 9 (Child and youth welfare), version of the Child and Youth Strengthening Act (KJSG), BGBl. I S. 1444, 09.06.2021
Civil Status Act (PStG), amended by Act of 18.12.2018 (BGBl. I S. 2635): introduction of the “diverse” option for persons with variations of sex development
[2]N. Garrelts, “Kassen und Warken uneinig bei Kostenerstattung von Hormonen fuer trans Menschen”, Tagesspiegel Background Gesundheit, 24.03.2026 (paywalled); background.tagesspiegel.de
[3]Tagesspiegel, Garrelts, 24.03.2026, ibid.: “She recommended concealing the non-binary status of patients from the health insurer, because this is often treated as grounds for exclusion.”
[4]Berlin District Court II, judgment of 10 March 2026, case no. 27 O 51/26 eV. Documentation: frauenheldinnen.de and

[5]A. Kroening, “’Absurd ethical conflicts,’ a resignation and the dispute about treatment costs”, Die Welt, 30.03.2026. welt.de
[6]T. Amelung, “After video leak and court ruling: Sabine Maur steps down from senior posts”, QueerNations, 24.03.2026. queernations.de
[7]WELT, Kroening, 12.02.2026: “Absurd ethical conflicts” - and how the insurer is still supposed to pay. welt.de
[8]bkj-ev.de and queernet-rlp.de and dgti.org
[9]Riki Anne Wilchins, “In Your Face” (newsletter of The Transsexual Menace), 1995.
[10]Earliest documented usage of “non-binary” around 2000: cf. J. Haynes / J. McKenna (eds.), Unseen Genders: Beyond the Binaries, New York 2001. S. Monro / D. Crocetti et al., “Non-binary and genderqueer: An overview of the field”, International Journal of Transgenderism 20(2-3), 2019.
[11]APA Division 44: “Given the underrepresentation of nonbinary gender populations in the literature, it is critical that psychologists add to the empirical base.” Cited in: Science for the People Magazine, Vol. 22(2), 2021.
[12]Cass Review, Final Report, NHS England, April 2024, pp. 28ff.
[13]AWMF S2k Guideline 028-014, March 2025. Guideline report: “The guideline does not contain evidence-based recommendations due to the overall uncertain evidence base.” Available: register.awmf.org/de/leitlinien/detail/028-014
[14]WPATH, Standards of Care, since 1979. SOC-8 (2022) assessed by the Cass Review (2024) as lacking “developmental rigour and transparency”. Available: wpath.org/publications/soc8
[15]DSM-5, APA, 2013: “gender dysphoria”. The only psychiatric diagnosis where diagnosis, treatment decision, and irreversible physical interventions are determined by patient self-report.
[16]AWMF S3 Guideline 138-001, October 2018. Valid until 08.10.2023, expired since then. Available: register.awmf.org/de/leitlinien/detail/138-001
[17]dgti e.V., commentary on the SOC-8 draft, January 2022. Available: dgti.org/2022/01/23/kommentar-zu-den-entwuerfen-der-standards-of-care-v8-soc-v8-der-wpath/
[18]ICD-11 (WHO, adopted May 2019, in force January 2022), code HA60. Not yet introduced into social law in Germany; the GKV operates on ICD-10 (F64.0). Available: icd.who.int
[19]FSC, judgment of 19.10.2023, B 1 KR 16/22 R, para. 18 and 24. Available: bsg.bund.de
[20]Commissioning letter, Federal Ministry of Health (Warken) to G-BA, 28.01.2026. Published via Frag den Staat. Available: fragdenstaat.de
[22]AWMF S2k Guideline 043-052, June 2025. See fn. 46 for detail. Available: register.awmf.org/de/leitlinien/detail/043-052
[23]FSC, ibid., para. 18: “The outpatient diagnosis including treatment planning and the subsequent inpatient treatment of the distress caused by gender incongruence through irreversible surgical interventions (here: mastectomy) constitutes a new method of examination and treatment within the meaning of Section 135 para. 1 sentence 1 SGB V.”
[24]Section 135 para. 1 sentence 1 SGB V: “New methods of examination and treatment may only be provided in the context of contract medical care at the expense of the health insurers if the Federal Joint Committee [...] has issued recommendations on the recognition of the diagnostic and therapeutic benefit [...] as well as its medical necessity and cost-effectiveness.”
[25]FSC, ibid., para. 24: “In the borderline area between illness within the meaning of the GKV and the personal identity protected under the general right of personality pursuant to Art. 2 para. 1 in conjunction with Art. 1 para. 1 of the Basic Law [...] it rests therefore first and foremost with the parliamentary legislature to regulate the statutory health insurance entitlements [...].” Available: bsg.bund.de
[26]Letter from Prof. Josef Hecken (G-BA) to Federal Minister Prof. Karl Lauterbach, 03.12.2024. Published via Frag den Staat, document no. 256809.
[27]Tagesspiegel Background Gesundheit, N. Garrelts, 26.06.2024: Hecken: “In the event of a benefit assessment, the evidence base would not have been sufficient to demonstrate a positive benefit for the various measures.”
[28]Letter from Prof. Josef Hecken (G-BA) to Federal Minister Prof. Karl Lauterbach, 29.11.2023. Published via Frag den Staat. Hecken proposed a new Section 27c SGB V.
[29]GKV-Spitzenverband, circular 2024-063, 31.01.2024. Published via Frag den Staat, document 245887.
[30]GKV-Spitzenverband, circular 2026/070, 03.02.2026. Published via Frag den Staat, IFG request 363649.
[31]Commissioning letter, Federal Ministry of Health (Warken) to G-BA, 28.01.2026. Available: fragdenstaat.de
[32]Commissioning letter, Warken, ibid.: “It is in particular its mandate to determine the scope of diagnostic and therapeutic treatment, without it being necessary for this purpose to conduct a complex and time-consuming benefit assessment procedure.”
[33]G-BA, press release “Selection of important work items for 2026”, 20.01.2026. The subject of gender incongruence is not mentioned with a single word.
[34]N. Garrelts, Tagesspiegel Background Gesundheit, 24.03.2026, ibid.
[35]Tagesspiegel Background, Garrelts, 24.03.2026, ibid. The G-BA began work on 19.03.2026.
[36]FSC, judgment of 19.10.2023, B 1 KR 16/22 R, para. 18ff. Available: bsg.bund.de
[37]G-BA, information sheet “Conditions for the provision of a (new) method at the expense of the GKV”, 2013. Available: g-ba.de.
[38]Section 116b para. 1 sentence 2 no. 2 letter i SGB V lists “transsexualism” (ICD-10 code F64.0). Non-binary identities are not listed.
[39]Coalition agreement 2025, CDU/CSU/SPD, “Responsibility for Germany”, April 2025. Published via Frag den Staat, document 258046.
[40]P. Rawee, R. Hartman et al., “Development of Gender Non-contentedness During Adolescence and Early Adulthood”, Archives of Sexual Behavior 53, 2024, pp. 2789-2802.
[41]U. Bachmann et al., “Gender identity disorders in young people in Germany: frequency and trends 2013-2022”, Deutsches Aerzteblatt International 121, 2024.
[42]S.-M. Ruuska, K. Tuisku, T. Holttinen, R. Kaltiala, “Psychiatric Morbidity Among Adolescents and Young Adults Who Contacted Specialised Gender Identity Services in Finland in 1996-2019: A Register Study”, Acta Paediatrica (2026), doi:10.1111/apa.70533.
[43]E. Reed, “Fact Check: New Finnish Study Does Not Prove Trans Youth Care Leads To Worse Outcomes”, erininthemorning.com, April 2026. The critique addresses surveillance bias; the core findings are not refuted.
[44]Tagesspiegel Background Gesundheit, N. Garrelts, 26.06.2024, ibid. Hecken verbatim: “The evidence is insufficient for a positive benefit assessment.”
[45]L. Woerner, A. Windsberger, V. Roessner, “Gender-affirming medical measures for minors as a violation of Section 1631c BGB? - A critical criminal law assessment”, ZfIStw 5/2025, pp. 1718ff.
[46]AWMF S2k Guideline 043-052 “Surgical Measures for Gender Incongruence”, June 2025. No minimum age for body-modifying interventions, no specific recommendations for non-binary persons. A survey referenced in the guideline found that 11 of 20 WPATH-associated US surgeons also operate on minors (AWMF 043-052, p. 31). The combination of mastectomy, hysterectomy, salpingo-oophorectomy, and colpectomy/colpoclesis amounts to complete removal of all primary and secondary female sex characteristics. Available: register.awmf.org/de/leitlinien/detail/043-052
[47]AWMF S2k Guideline 028-014, March 2025. Trans organizations submitted a dissenting opinion calling for mastectomies in minors regardless of binary character of gender identity - contrary to the guideline’s actual recommendation. Available: register.awmf.org/de/leitlinien/detail/028-014
[48]dgti e.V., Qualitaetszirkel Psychotherapeut*innen, since January 2023: “The meetings of the quality circle are certified by the LPK RLP; 3 continuing education points are currently awarded (valid nationwide). The costs for registration for certification are currently borne by the dgti.” Available: dgti.org/2023/01/03/qualitaetszirkel-psychotherapeutinnen/
[49]IGLYO / Dentons / Thomson Reuters Foundation, “Only Adults? Good Practices in Legal Gender Recognition for Youth”, November 2019. Available: iglyo.com
[50]Rona Duwe, “She wanted to silence me. She got a verdict.”, Substack ronalyze, 2026. Available:
[51]TransTeens Sorge berechtigt (TTSB), “GKV-Erstattung: Der G-BA soll den gordischen Knoten loesen”, 27.03.2026. Available: transteens-sorge-berechtigt.net
[52]FSC, ibid., para. 24: “In the borderline area between illness within the meaning of the GKV and the personal identity protected under the general right of personality pursuant to Art. 2 para. 1 in conjunction with Art. 1 para. 1 of the Basic Law [...] it rests therefore first and foremost with the parliamentary legislature to regulate the statutory health insurance entitlements [...].”